")

My Doctor Said I Just Need Better Sleep Hygiene. Why Isn’t It Working?
You’ve done everything right. The room is dark. The phone is off. You switched to decaf three months ago. You bought the weighted blanket, the blackout curtains, the magnesium supplements. You have a bedtime routine so precise it could be published as a protocol.
And yet here you are, wide awake at 2am, staring at the ceiling, wondering what you’re still getting wrong.
If your sleep hygiene isn’t working for insomnia, there’s something you should know: you’re not broken, and you’re not doing it wrong. You’re using a tool that was never designed for the problem you actually have. That distinction matters, because the treatment that does work looks completely different from anything on a sleep hygiene checklist. And once you understand why, a lot of the frustration starts to make sense.
 What Is Sleep Hygiene, and What Is It Actually Good For?
What Is Sleep Hygiene, and What Is It Actually Good For?
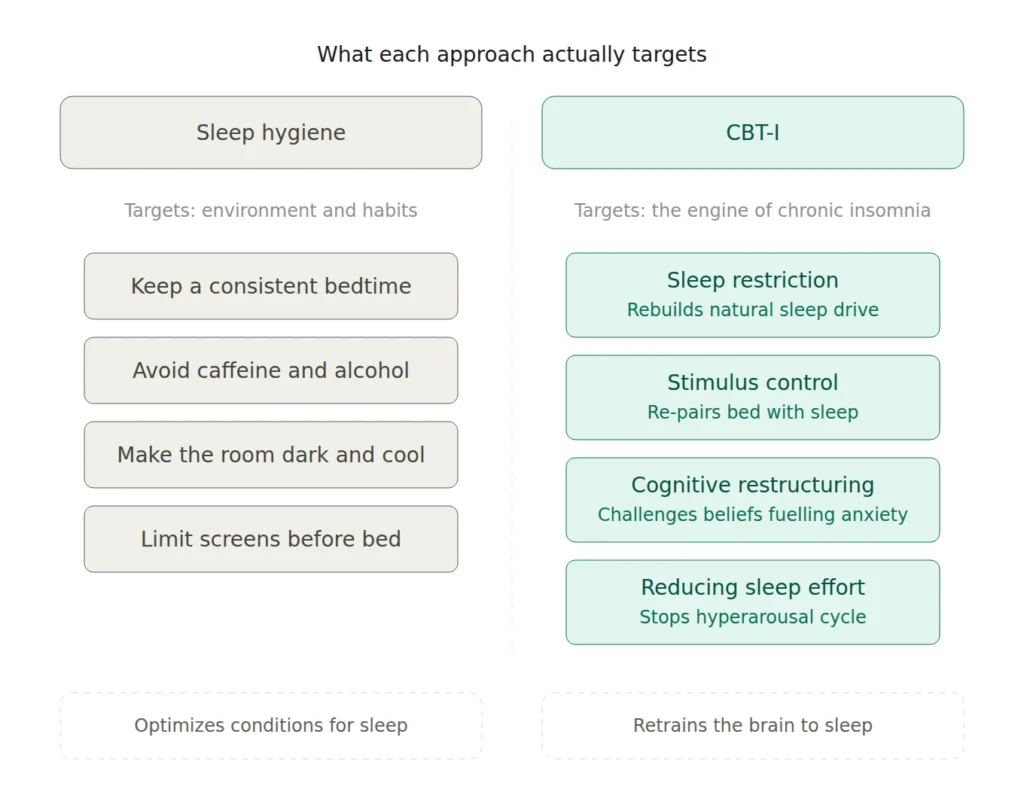
Sleep hygiene is a set of behavioural and environmental recommendations meant to support healthy sleep. Keep a consistent schedule. Exercise during the day. Avoid caffeine and alcohol in the evening. Make the bedroom cool, dark, and quiet. Limit screen time before bed.
These are perfectly sensible guidelines. For someone whose sleep has been thrown off by a stretch of late nights, a new coffee habit, or a noisy apartment, tidying up these basics can genuinely help. If you’re a generally decent sleeper going through a rough patch, sleep hygiene gives your system the best conditions to do what it already knows how to do.
But here’s the catch. If you’ve had insomnia for months or years, if you’ve already followed every tip on the list and you’re still struggling, then the problem isn’t your environment. The problem is deeper than that. And no amount of environmental optimization is going to reach it.
Why Is Sleep Hygiene Not Working for Your Insomnia?
To understand why sleep hygiene falls short, it helps to understand how insomnia develops in the first place.
Sleep Hygiene Targets the Wrong Part of the Problem
In the 1980s, sleep researcher Arthur Spielman introduced what’s now known as the 3P model of insomnia. It describes three sets of factors that contribute to the disorder: predisposing factors (traits that make you vulnerable, like genetics or a tendency to worry), precipitating factors (the stressor that triggers the first bad stretch of sleep), and perpetuating factors (the behaviours and thought patterns that keep insomnia alive long after the original trigger has passed).
This is where most people get stuck. The precipitating event, the thing that started it all, might be long gone. The work deadline passed. The relationship settled. The health scare resolved. But insomnia stayed, because a new set of factors quietly moved in and took over.
Perpetuating factors include things like spending extra time in bed to “catch up,” napping during the day, going to bed before you’re sleepy, and developing anxious thoughts about what another bad night will do to you. These are the behaviours that keep the cycle spinning. And sleep hygiene doesn’t touch any of them.
Sleep hygiene addresses the precipitating layer. It’s designed to remove external interference with sleep. But for chronic insomnia, the interference is no longer external. It’s internal: conditioned arousal, learned associations, and a nervous system that has started treating wakefulness in bed as the default.
The Harder You Try to Sleep, the Harder Sleep Becomes
Here’s the part that nobody tells you, and it’s a little maddening. When sleep hygiene becomes a rigid, high-stakes performance, it can actually make insomnia worse.
Think about the people you know who sleep well. If you asked them what they do to fall asleep, most of them would shrug. They don’t have a protocol. They don’t time their last sip of water. They just… go to bed. Sleep, for them, isn’t something they manage. It’s something that happens.
Now think about what insomnia does to your relationship with sleep. It turns it into a project. Every evening becomes a rehearsal. Every choice (did I eat too late? Was the room warm enough? Should I have skipped that TV episode?) gets filtered through the question: will this help me sleep tonight?
That vigilance is the problem. The more you monitor, optimize, and try to control sleep, the more your brain treats sleep as something fragile and dangerous. This feeds a kind of hyperarousal that keeps the system alert precisely when it needs to stand down. Many of the people I work with arrive having turned sleep hygiene into a second job. They’ve become so disciplined about sleep that the discipline itself is what’s keeping them awake.
What Does the Research Actually Say About Sleep Hygiene for Insomnia?
This isn’t just a clinical hunch. The evidence is clear, and it has been for a while.
The American Academy of Sleep Medicine’s 2021 clinical practice guideline explicitly recommends against using sleep hygiene as a standalone treatment for chronic insomnia. The guideline notes that while sleep hygiene practices are commonly suggested and well understood by patients, they do not constitute an effective treatment on their own. The recommendation is to use sleep hygiene only as part of a broader, multicomponent approach.
Sleep researchers have known this for so long that sleep hygiene education is routinely used as the control condition in insomnia treatment trials. In research terms, that makes it the equivalent of a placebo. As Scientific American put it, sleep hygiene performs so poorly as a standalone intervention that researchers use it as the baseline against which real treatments are measured.
A 2025 systematic review and meta-analysis published in Sleep Medicine Reviews looked at 42 randomized controlled trials involving over 4,200 adults. The findings confirmed that sleep hygiene education was significantly less effective than CBT-I, partial CBT-I, exercise, and even acupressure for reducing insomnia severity.
None of this means sleep hygiene is useless. It has its place as a foundation, a set of reasonable habits that support good sleep. But treating it as a solution for chronic insomnia is like telling someone with a broken leg to buy better shoes. The shoe isn’t the problem.
What Is CBT-I, and Why Is It Categorically Different?
If sleep hygiene targets the surface, Cognitive Behavioural Therapy for Insomnia (CBT-I) goes after the engine that keeps insomnia running.
How Does CBT-I Actually Treat Insomnia?
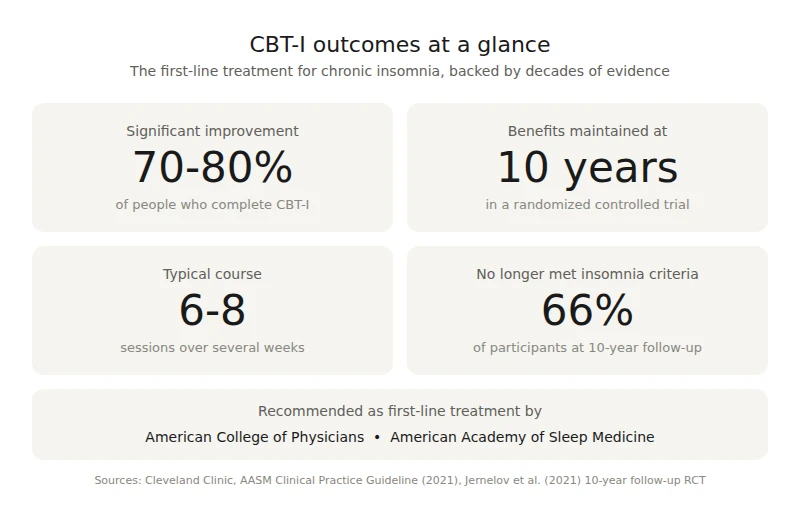
CBT-I is a structured, evidence-based treatment typically delivered over six to eight sessions. It directly targets the perpetuating factors that Spielman’s model identifies as the drivers of chronic insomnia.
The core components include sleep restriction (compressing your time in bed to match the amount of sleep you’re actually getting, which rebuilds sleep drive), stimulus control (re-establishing the bed as a cue for sleep rather than wakefulness), and cognitive restructuring (identifying and challenging the unhelpful beliefs about sleep that fuel anxiety at bedtime). You can read more about what CBT-I actually teaches you about sleep and why it looks nothing like a list of tips.
Where sleep hygiene says “make your room darker,” CBT-I says “let’s figure out why your brain has learned to be alert in bed, and retrain it.” It’s the difference between adjusting the scenery and rewiring how CBT-I works to treat chronic insomnia at its source.
How Effective Is CBT-I Compared to Sleep Hygiene or Medication?
The numbers are striking. According to the Cleveland Clinic, seven to eight out of ten people who complete CBT-I show significant improvement in their sleep. The American College of Physicians and the AASM both recommend it as the first-line treatment for chronic insomnia in adults.
And unlike medication, the benefits tend to last. A randomized controlled trial with a 10-year follow-up found that improvements from CBT-I were well maintained a full decade after treatment. Two-thirds of participants no longer met criteria for an insomnia diagnosis at the 10-year mark. Sleep medication, by contrast, typically works only as long as you take it, and long-term use raises concerns around dependency and side effects.
CBT-I doesn’t just reduce symptoms. It restores your body’s natural capacity to sleep by addressing the patterns that were overriding it.
If CBT-I Is So Effective, Why Did My Doctor Only Suggest Sleep Hygiene?
This is a fair question, and it’s not about blame. Most family doctors receive very little training in behavioural sleep medicine. Sleep hygiene and medication are often the only tools in the toolkit, not because they’re the best options, but because they’re the most accessible ones.
There is also a significant shortage of trained CBT-I providers. Patients are far more likely to hear about sleep medication through advertising and prescriptions than they are to be referred to a CBT-I therapist. The result is a gap between what the evidence recommends and what most people are actually offered. The AASM has pointed to this as a systemic issue, noting that CBT-I’s widespread dissemination has not kept pace with the evidence supporting it.
This is starting to change. More clinicians are becoming aware of CBT-I as the recommended first-line treatment, and online delivery has expanded access considerably. But for now, many people with chronic insomnia still spend years cycling through sleep hygiene advice and prescriptions before finding out that a structured, time-limited therapy exists.
What Should You Do Next If Sleep Hygiene Isn’t Enough?
If you’ve been doing all the “right things” and your insomnia hasn’t budged, here are some practical next steps.
First, recognize that this is a signal, not a sentence. Chronic insomnia that doesn’t respond to sleep hygiene is telling you something useful: the problem has moved past the point where environmental adjustments can reach it. That’s not a reflection of how severe your insomnia is. It’s a reflection of what kind of treatment it needs.
Second, look for a therapist trained in CBT-I. A typical course of treatment runs six to eight sessions, and it can be delivered effectively online, which is especially relevant if you’re in a smaller community or a region where providers are limited. In British Columbia, you don’t need a referral from your doctor to begin.
Third, know that CBT-I can feel counterintuitive at first. Sleep restriction, in particular, means temporarily spending less time in bed, which sounds backwards when you’re already exhausted. But it works by rebuilding the sleep pressure your body needs to fall asleep efficiently. The discomfort is short-lived; the results tend to stick.
You’re Not Failing at Sleep. You Just Need a Different Approach.
If sleep hygiene hasn’t worked for your insomnia, that’s not a failure on your part. It means your sleep difficulty has developed its own momentum, driven by patterns that no amount of blackout curtains or herbal tea can interrupt. The reassuring part is that those patterns are well understood, and the treatment designed to address them is one of the most effective interventions in all of behavioural medicine.
CBT-I is structured, time-limited, and backed by decades of evidence. It doesn’t ask you to try harder at the things that aren’t working. It gives you an entirely different set of tools, ones that target the actual mechanics of why your sleep isn’t functioning the way it should.
If you’re ready to stop managing insomnia and start treating it, book a free consultation with BC CBT-I. We work with people across British Columbia, online, to help you get your sleep back without medication and without another checklist.
