")

The Jobs Most Likely to Give You Insomnia in BC (And What Actually Helps)
British Columbia runs on people who work hard, often at odd hours, in conditions that demand a lot. Nurses on overnight rotations. Firefighters waiting for the next call. Teachers carrying thirty kids’ worth of worry home in their heads. Managers checking their phones at midnight.
These are some of the most essential workers in the province. They’re also, not coincidentally, some of the most likely to develop insomnia.
That’s not a complaint about their jobs. It’s a structural observation. Certain kinds of work create conditions that are genuinely incompatible with good sleep. Not because the people doing them are doing anything wrong, but because of what those jobs ask of the brain and body. Understanding that distinction matters, because it changes what you do about it.
This post covers the professions with the highest insomnia rates, why each one tends to produce sleep problems in specific ways, and what the evidence actually says about treatment.
 Insomnia Is More Common in the Workforce Than Most People Realise
Insomnia Is More Common in the Workforce Than Most People Realise
Before getting into occupations specifically, it’s worth grounding this in the Canadian picture.
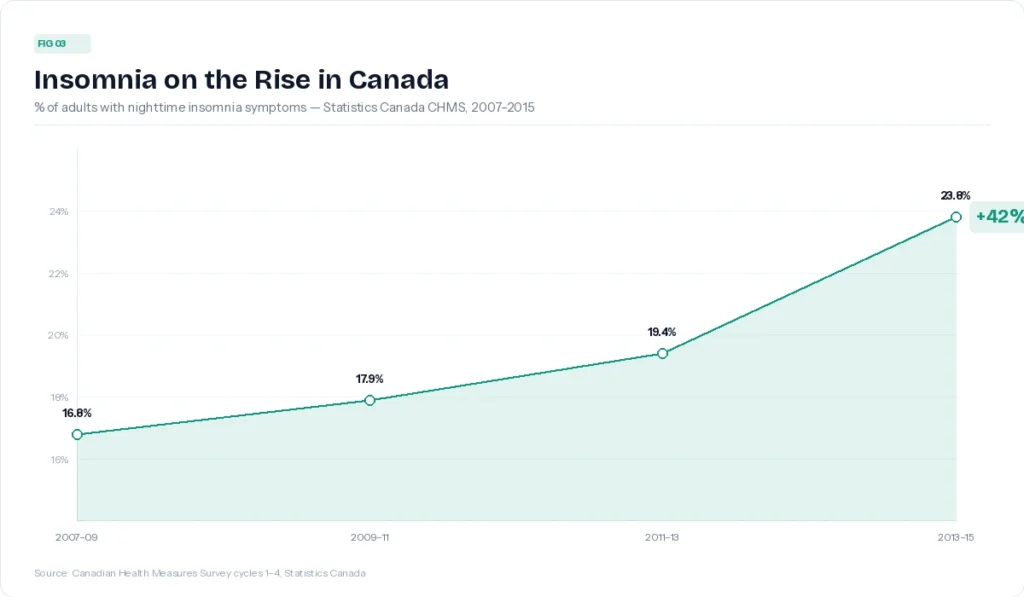
Statistics Canada data show that insomnia symptoms among Canadian adults rose by 42% between 2007 and 2015. A more recent national survey puts the prevalence of full clinical insomnia disorder at around 16.3% of Canadian adults, meaning roughly one in six people meets the diagnostic criteria on duration, frequency, and daytime impairment.
These aren’t people who occasionally have a bad night. Clinical insomnia means struggling to fall or stay asleep at least three nights a week for at least three months, with real consequences during the day. That’s a meaningful bar, and a lot of Canadians are clearing it.
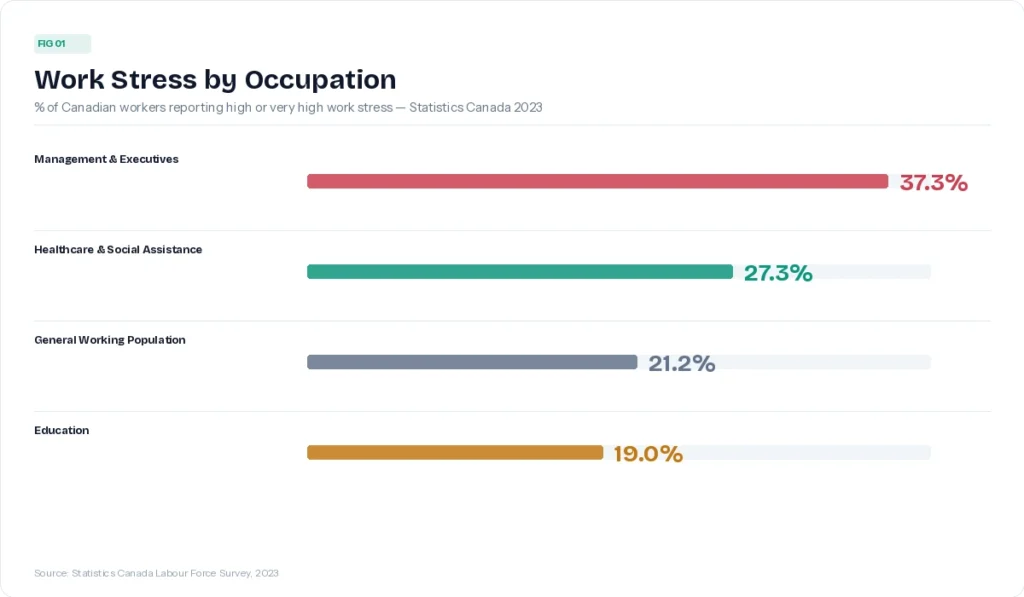
Work is one of the most consistent predictors. A Statistics Canada analysis of employed Canadians found that 21.2% of the working population reported high or very high work-related stress. And not all jobs carry that burden equally.
 The Jobs Most Likely to Give You Insomnia
The Jobs Most Likely to Give You Insomnia
Healthcare Workers and Nurses
Healthcare and social assistance workers have the highest work-stress rates of any sector in Canada at 27.3%, with nearly a third citing heavy workload and over a fifth citing emotional load specifically.
For nurses, the picture is sharpened by shift work. Research shows that around 40% of night-shift nurses show symptoms consistent with shift work disorder, which includes difficulty sleeping, excessive sleepiness, and insomnia. Night-shift nurses average only 5.7 hours of sleep compared to 6.7 hours for their daytime colleagues. Few reach the recommended seven to eight hours during recovery periods.
The core problem is circadian. The human sleep-wake cycle is regulated by light exposure, mealtimes, and social timing. Rotating shift work constantly disrupts that system. The body tries to adapt and mostly can’t. Even nurses who have worked nights for years rarely achieve full circadian alignment, partly because they revert to a daytime schedule on days off.
There’s also the emotional weight. Healthcare work involves sustained proximity to suffering, high-stakes decisions, and moral strain. That kind of load doesn’t clock out when the shift ends. It tends to follow people home in the form of rumination, which is one of the more reliable pathways to chronic insomnia.
First Responders: Firefighters, Paramedics, and Police Officers
A systematic review drawing on data from over 100,000 first responders found that 28% meet criteria for insomnia, alongside similarly high rates of shift work disorder and excessive daytime sleepiness.
The mechanisms here are layered. Shift work and unpredictable call patterns disrupt circadian rhythms in the same way they do for nurses. But first responders face an additional factor: occupational hypervigilance. A brain trained to stay alert for threats has a harder time shifting into the relaxed, lower-arousal state that sleep requires. That’s not a character flaw. It’s the nervous system doing exactly what the job trained it to do.
Repeated trauma exposure adds another layer. For first responders with PTSD or significant trauma load, fear of sleep itself can emerge as a clinical issue, compounding insomnia through nightmares, nocturnal vigilance, and conditioned arousal around bedtime. The relationship between trauma, PTSD, and insomnia is bidirectional: poor sleep worsens trauma symptoms, which in turn makes sleep harder. You can read more about how chronic stress and trauma interact with insomnia and what trauma-informed treatment looks like.
Teachers
Teachers often get left off these lists, which is puzzling given what the research shows. Compared to the general working population, teachers face greater occupational stress and are more prone to insomnia. Studies consistently find that 55 to 61% of teachers report poor sleep quality. In one survey, nearly a quarter reported that daily activities were impaired by sleepiness, and 43% slept six hours or less per night.
Teaching is cognitively and emotionally demanding in ways that are easy to underestimate from the outside. The work involves constant emotional labour, managing thirty different personalities while also tracking curriculum demands, administrative requirements, and any number of family situations that show up in the classroom. And unlike shift work, the circadian disruption isn’t the main culprit here. For teachers, it’s typically rumination. The replay of a difficult interaction. Worrying about a student. Grading in your head at 1 a.m.
Research on teacher sleep quality found that experiences of failure at work, emotional dissonance, and social exclusion at work were the most consistent predictors of sleep problems. Teachers who could psychologically detach from work during their off-hours slept significantly better. The problem is that psychological detachment, when the work involves real children and real stakes, is genuinely hard to achieve.
Managers and Executives
Statistics Canada data place management-level workers at the top of the occupational stress ladder, with 37.3% reporting high or very high work stress. This is the highest rate of any occupational category measured.
The insomnia risk in management tends to be driven less by circadian disruption and more by what researchers call the effort-reward imbalance: a chronic mismatch between the effort and responsibility the job demands and the sense of control, recognition, or reward received. When that imbalance persists, the threat response stays engaged. And an engaged threat response is not compatible with restful sleep.
There’s also the always-on culture. For many managers and executives, the boundary between work and rest has become genuinely porous. The research on psychological detachment is consistent: workers who mentally disengage from work during leisure time report better sleep quality, mood, and energy. When work content occupies the mental foreground in the evening, cognitive arousal stays elevated well past the time it would need to drop for sleep to begin.
 Why Does Your Job Actually Cause Insomnia?
Why Does Your Job Actually Cause Insomnia?
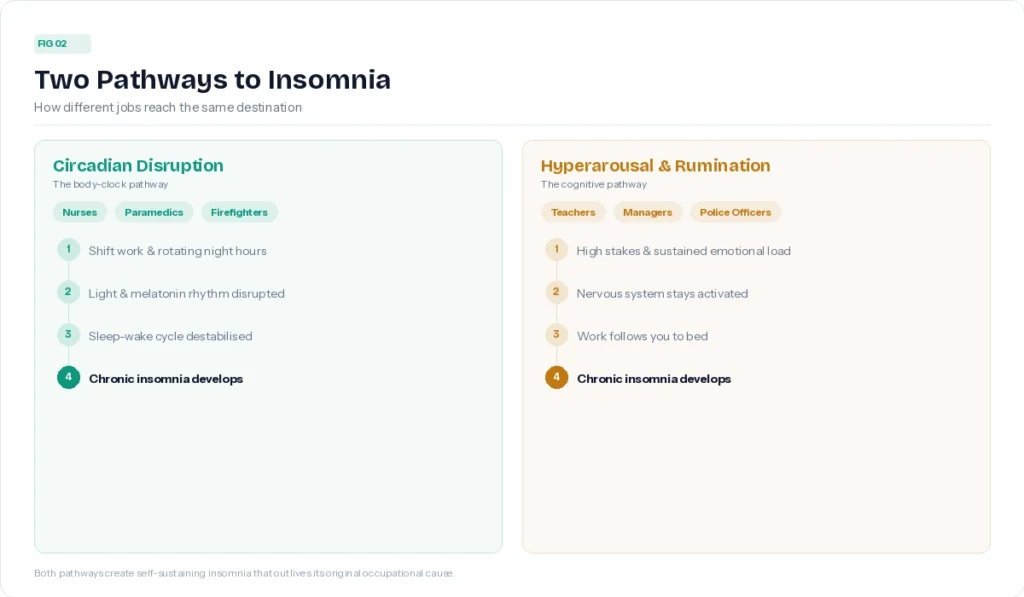
Most occupational insomnia traces back to one of two mechanisms, or a combination of both.
The first is circadian disruption. The sleep-wake cycle is a biological system, not just a preference. It’s governed by light exposure, cortisol rhythms, body temperature, and melatonin timing. When work schedules repeatedly override that system, whether through night shifts, rotating hours, or irregular patterns, the body loses its anchor. Sleep becomes harder to initiate, less restorative, and more fragmented.
The second is hyperarousal. This is the nervous system’s version of leaving the engine running. It can show up as physical tension, racing thoughts, heightened alertness at bedtime, or the kind of cognitive rumination that makes lying down feel like an invitation for every unresolved work problem to surface at once. Hyperarousal is common across high-stress occupations, but it tends to be especially prominent in roles that involve high stakes, emotional labour, or trauma exposure.
What makes occupational insomnia clinically significant is that it often becomes self-sustaining. The job may have triggered the sleep problem, but over time, insomnia develops its own logic. The bed becomes associated with wakefulness. Anxiety about sleep compounds the original arousal. The original occupational stressor and the insomnia start operating as separate, mutually reinforcing problems.
Does Fixing Your Sleep Hygiene Actually Help?
This is the honest question, and it deserves a direct answer.
Sleep hygiene, meaning the standard advice about screens, caffeine, consistent schedules, and a cool dark room, can reduce friction. For someone with mild or occasional sleep difficulty, it’s reasonable first-line guidance. But for someone with established clinical insomnia rooted in occupational stress, it typically isn’t enough.
Here’s why. Sleep hygiene addresses the conditions around sleep. It doesn’t address the arousal system that’s keeping you awake, the conditioned wakefulness you’ve built up over months of lying awake in your bed, or the cognitive patterns, worry, catastrophising about sleep, clock-watching, that perpetuate insomnia long after the original trigger has settled down.
People in high-stress occupations often try every sleep hygiene recommendation and still can’t sleep. That’s not a failure of willpower. It’s a sign that what they’re dealing with is more than hygiene-level. Why therapy is often the missing piece in treating insomnia comes down to this: the brain needs more than environmental adjustments. It needs the underlying arousal system addressed.
What Actually Works for Occupational Insomnia
The evidence consistently points to Cognitive Behavioural Therapy for Insomnia (CBT-I) as the first-line treatment for chronic insomnia, including insomnia with an occupational cause. It’s recommended ahead of sleep medication by sleep medicine bodies in Canada and internationally, not as a consolation prize, but because it produces more durable results.
CBT-I works by targeting the three systems that maintain insomnia: sleep drive (the biological pressure that builds through waking hours), the circadian clock (the timing system that regulates when you feel sleepy), and arousal (the psychological and physiological activation that interferes with sleep onset and maintenance). It also addresses the thoughts and behaviours around sleep that develop over time and keep the problem going independent of the original cause.
For workers in high-stress or trauma-exposed roles, CBT-I is often combined with elements of Acceptance and Commitment Therapy (ACT). ACT doesn’t try to eliminate anxious thoughts about sleep. It changes your relationship to them, reducing the struggle and the secondary distress that magnifies insomnia’s hold. A comprehensive overview of how CBT-I and ACT work together covers the full picture of what treatment involves.
The important thing to understand is this: even when you can’t change your job, you can change how insomnia develops in response to it. The occupational stressor may have been the trigger. But insomnia, once established, operates by its own rules, and those rules can be interrupted.
If you’re curious about what taking that step actually looks like in practice, a walkthrough of what happens in a first CBT-I session is a good starting point.
You Can’t Pour From an Empty Cup (But You Already Know That)
If you’re in one of these professions, you’ve probably heard that phrase before. You’ve probably said it to someone else. And you’re probably also familiar with the particular exhaustion of knowing something intellectually and still not doing it.
Sleep isn’t a luxury for people in demanding work. It’s what makes everything else possible. The quality of the care you give, the decisions you make, the emotional reserves you draw on at the end of a hard shift: all of it rests on how well your brain is recovering at night.
If your job is costing you sleep, and sleep tips haven’t helped, it may be time to look at a more targeted approach. CBT-I is available in BC, online, and specifically designed for people whose insomnia has become bigger than its original cause.
Book a free 15-minute consultation to find out whether CBT-I is the right fit for where you’re at.
